















Instructional Video
How to Safely Taper Antipsychotics
Summary
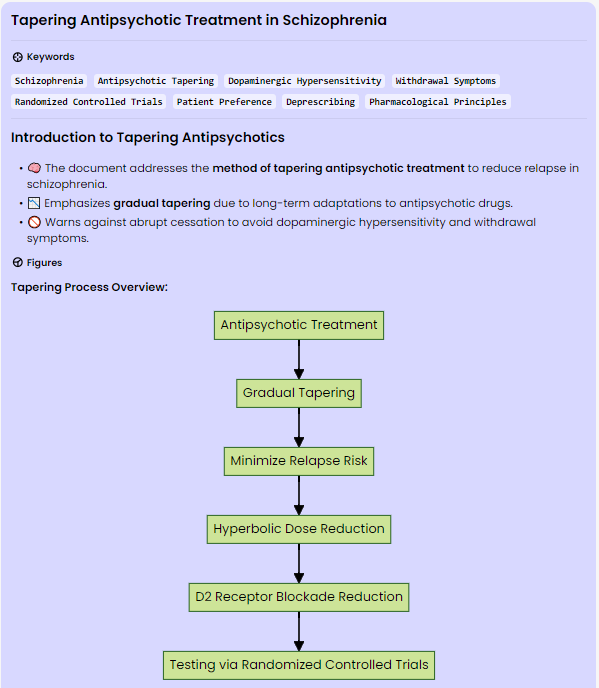
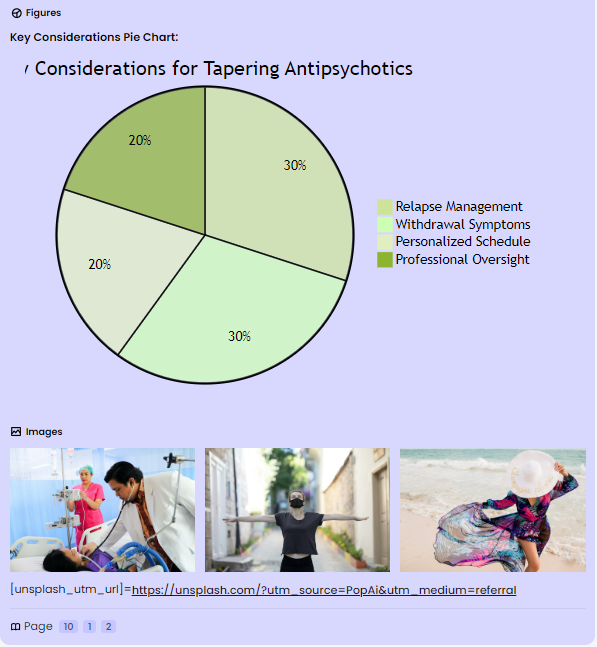
The document discusses a method for tapering antipsychotic treatment to minimize the risk of relapse in patients with schizophrenia. It emphasizes the need for gradual tapering due to the persistence of adaptations to antipsychotic exposure, potentially leading to dopaminergic hypersensitivity and withdrawal symptoms upon cessation. The paper suggests a tapering approach that reduces antipsychotic doses gradually and in a hyperbolic manner to evenly reduce D2 receptor blockade. It recommends reducing by one quarter or one half of the most recent dose, at intervals of 3-6 months, with final doses before complete cessation as small as 1/40th of the therapeutic dose. The proposal advocates testing this method in randomized controlled trials, highlighting the significance of tailoring the tapering process to individual tolerance and preferences.
The introduction underscores the increasing emphasis on patient preference and shared decision-making in the context of deprescribing antipsychotic medication. It points out the uncertainty surrounding the need for long-term antipsychotic use in schizophrenia and the potential benefits of attempting reduction or cessation of antipsychotics in patients who have remitted after treatment. The document highlights the relevance of withdrawal syndromes and their association with abrupt cessation of antipsychotics, emphasizing the need for a methodical and individualized tapering approach.
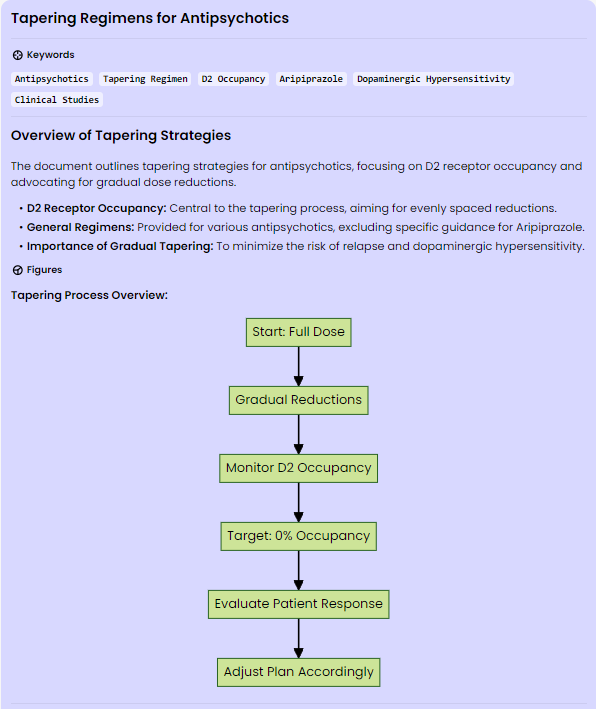
Furthermore, the document delves into the neurobiological and pharmacological aspects of antipsychotic withdrawal syndrome, including the role of dopaminergic hypersensitivity and withdrawal-associated psychosis. It discusses the evidence supporting prolonged tapering to minimize relapse rates, citing meta-analyses and randomized controlled trials. The proposed tapering regimens for various antipsychotics are detailed, emphasizing the importance of pharmacologically informed tapering to optimize clinical outcomes.
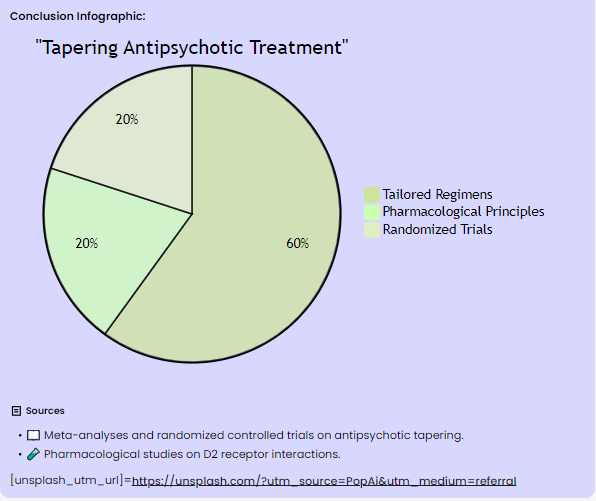
In conclusion, the document provides a comprehensive overview of the rationale for and approach to tapering antipsychotic treatment to minimize the risk of relapse. It emphasizes the need for tailored and gradual tapering regimens, informed by pharmacological principles, to address the challenges associated with antipsychotic withdrawal and to optimize patient outcomes. The proposal encourages further research through randomized controlled trials to validate the efficacy of the suggested tapering method.
What are the proposed principles for reducing and discontinuing antipsychotics in a manner that minimizes the risk of relapse?
The proposed principles for reducing and discontinuing antipsychotics in a manner that minimizes the risk of relapse include the following:
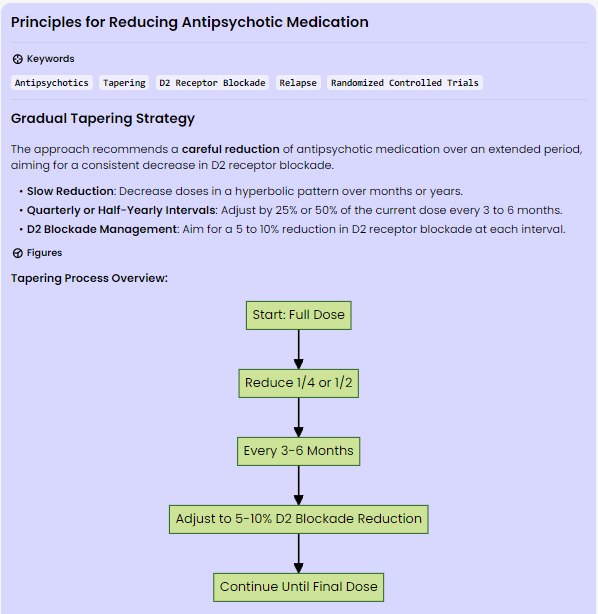
1. Gradual Tapering: The document suggests reducing antipsychotic doses gradually over months or years and in a hyperbolic manner to reduce D2 receptor blockade evenly. This involves reducing by one quarter or one half of the most recent dose of antipsychotic, equivalent to a reduction of 5 or 10 percentage points of its D2 blockade, at intervals of 3–6 months, titrated to individual tolerance.
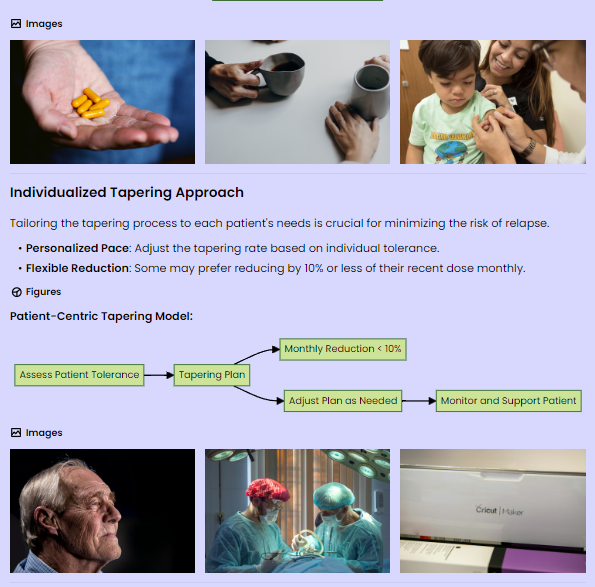
2. Individualized Tapering: The tapering process should be tailored to individual tolerance, and some patients may prefer to taper at 10% or less of their most recent dose each month.
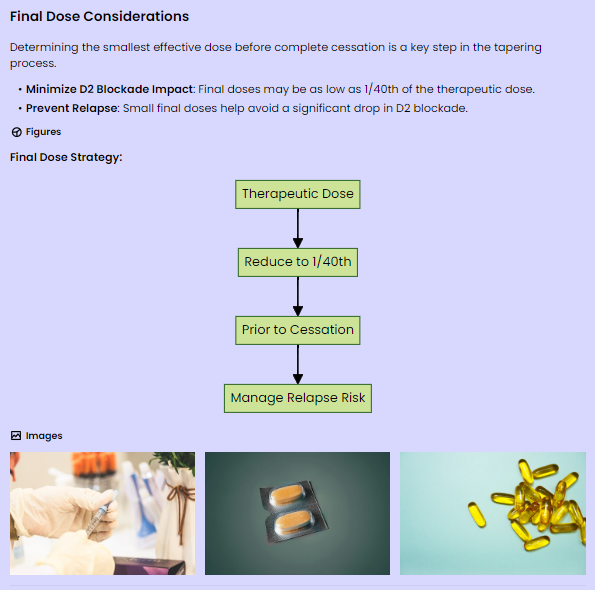
3. Final Doses: Final doses before complete cessation may need to be as small as 1/40th of a therapeutic dose to prevent a large decrease in D2 blockade when stopped.
4. Testing in Randomized Controlled Trials: The proposal advocates testing this method in randomized controlled trials to validate its efficacy. These principles aim to allow underlying adaptations time to resolve, possibly reducing the risk of relapse on discontinuation and should be tested in further tapering trials of antipsychotics, including slower tapering down to lower final doses before complete cessation.
What evidence supports the notion that longer tapering periods may lead to lower relapse rates compared with more rapid tapering periods?
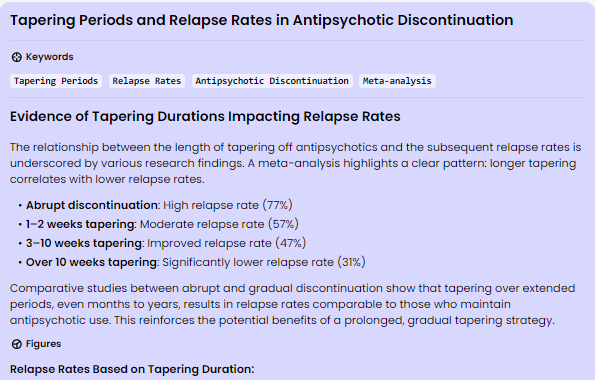
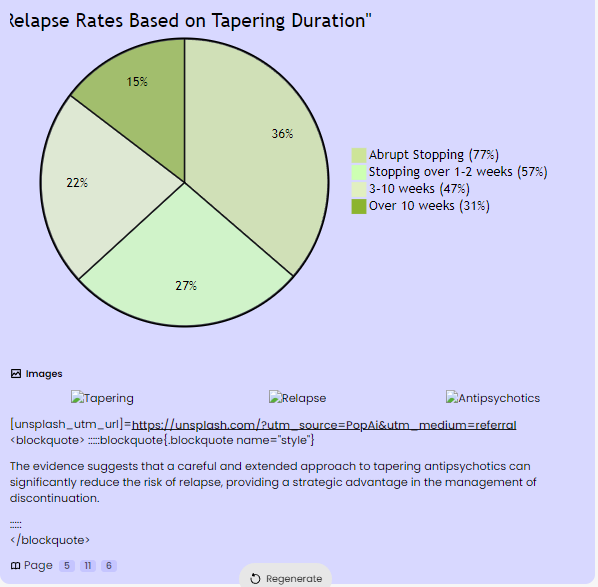
The evidence supporting the notion that longer tapering periods may lead to lower relapse rates compared with more rapid tapering periods is based on several studies and meta-analyses. A meta-analysis found an inverse dose response between the duration of discontinuation and the rate of relapse over the next year: abrupt stopping led to relapse in 77% of patients; stopping over 1–2 weeks led to relapse in 57%; 3–10 weeks to 47%; and stopping over longer than 10 weeks led to a relapse rate of 31%. Additionally, studies examining relapse rates comparing abrupt discontinuation with gradual discontinuation found that tapering over months and years down to small portions of drug doses demonstrated no significant difference in relapse rates between patients who continued or discontinued antipsychotics. These findings suggest that prolonged tapering periods may lead to lower relapse rates, supporting the notion that gradual tapering over an extended period may be more effective in minimizing the risk of relapse.
What are the recommended tapering regimens for six antipsychotics, based on D2 occupancy and evenly spaced reductions down to 0% occupancy?
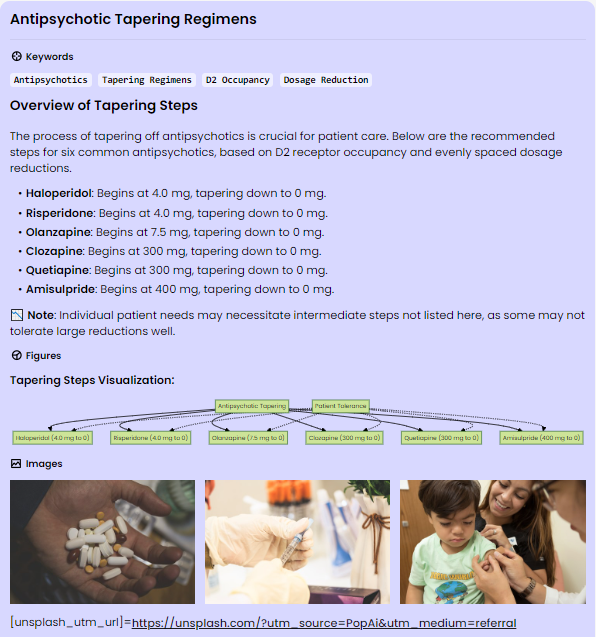
The recommended tapering regimens for six antipsychotics, based on D2 occupancy and evenly spaced reductions down to 0% occupancy, are as follows:
1. Haloperidol: - Starting from 4.0 mg, the tapering steps are: 4.0, 2.0, 1.3, 0.85, 0.60, 0.40, 0.25, 0.15, 0.05, 0.
2. Risperidone: - Starting from 4.0 mg, the tapering steps are: 4.0, 2.5, 1.7, 1.2, 0.85, 0.60, 0.40, 0.25, 0.10, 0.
3. Olanzapine: - Starting from 7.5 mg, the tapering steps are: 7.5, 5.9, 4.6, 3.6, 2.7, 2.0, 1.4, 0.90, 0.40, 0.
4. Clozapine: - Starting from 300 mg, the tapering steps are: 300, 210, 150, 110, 80, 55, 40, 25, 10, 0.
5. Quetiapine: - Starting from 300 mg, the tapering steps are: 300, 240, 200, 160, 120, 90, 65, 40, 20, 0.
6. Amisulpride: - Starting from 400 mg, the tapering steps are: 400, 270, 190, 140, 95, 70, 45, 25, 10, 0.
These tapering regimens are based on D2 occupancy and involve evenly spaced reductions to gradually reduce the antipsychotic dose down to 0% occupancy. It is important to note that individual patients may require intermediate steps between the values shown, as the reductions may represent too large a reduction for some patients to easily tolerate. Therefore, the reduction rate should be titrated to the ability of the patient to tolerate reductions.
How can the tapering process be individualized, and what are the potential challenges and considerations for tapering patients who have received long-term antipsychotics?
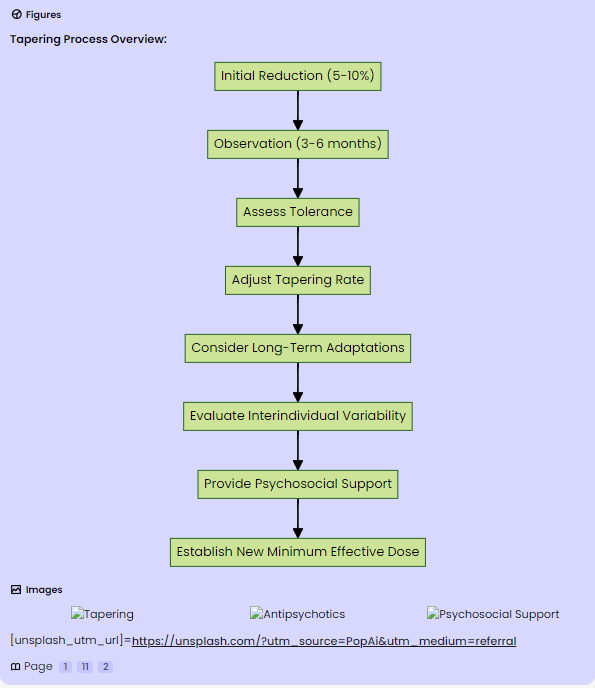
The tapering process can be individualized by observing patients for 3-6 months following an initial reduction of 5-10 percentage points of D2 receptor blockade and gauging their response to determine a tolerable rate of decrease thereafter. This individualized approach allows for the assessment of each patient's tolerance and response to the tapering process, enabling adjustments to be made based on their specific needs and reactions.
For patients who have received long-term antipsychotics, there are several potential challenges and considerations for tapering. These include the need for prolonged tapering periods to minimize the risk of psychotic relapse, as adaptations to antipsychotics can persist for many years. The tapering process may need to be prolonged to allow for the resolution of underlying adaptations, which can take weeks or even months. Additionally, there is considerable interindividual variability in the tapering process, with some patients requiring longer periods due to the persistence of adaptations, while others may tolerate shorter tapering periods.
Furthermore, patients with poor compliance may find prolonged tapers challenging, and increased psychosocial support may be necessary to manage this period. It is also important to consider the potential increase in symptoms following a dose reduction, which may resolve over time as underlying adaptations resolve. Increased psychosocial support may be necessary to manage this period if risks are manageable.
Overall, the tapering process should be conceptualized as finding a new minimum effective dose, and it may require adjustments based on individual patient responses and tolerances. It is essential to consider the potential challenges and individual variability when tapering patients who have received long-term antipsychotics.
What are the recommended tapering regimens for Aripiprazole and evenly spaced reductions down to 0% occupancy?
The document provides tapering regimens for various antipsychotics based on D2 occupancy and evenly spaced reductions down to 0% occupancy. However, it does not specifically outline a tapering regimen for Aripiprazole based on D2 occupancy and evenly spaced reductions down to 0% occupancy. The document does mention that drugs like Aripiprazole, which are partial agonists at the D2 receptor, are less likely to induce dopaminergic hypersensitivity and may be less likely to cause a relapse on discontinuation, as supported by animal data. However, it notes that this has not yet been examined in clinical studies.
Given the lack of specific tapering regimens for Aripiprazole based on D2 occupancy and evenly spaced reductions down to 0% occupancy in the provided document, it is important to consult with a healthcare professional for guidance on tapering Aripiprazole and to consider individual patient responses and tolerances when developing a tapering plan.

Safely tapering antipsychotics in Simple Steps
Safely tapering antipsychotics involves a gradual reduction of the medication to minimize the risk of relapse and withdrawal symptoms. Here are the simple steps to safely taper antipsychotics:
1. Initial Assessment: Begin with an initial reduction of 5-10% of D2 receptor blockade and monitor the patient's response for 3-6 months.
2. Gradual Reduction: Reduce the antipsychotic dose gradually over months or years in a hyperbolic manner, aiming for a reduction of 5-10% of D2 blockade at each interval.
3. Individualized Approach: Tailor the tapering plan to each patient's tolerance and response, adjusting the tapering rate based on individual needs.
4. Final Dose: Before complete cessation, the final doses should be as small as 1/40th of the therapeutic dose to prevent a significant decrease in D2 blockade.
5. Professional Guidance: Always consult with a healthcare professional to develop a safe and effective tapering plan tailored to the patient's specific needs.
By following these steps, patients can safely taper off antipsychotic medication while minimizing the risk of relapse and withdrawal symptoms.
Safely tapering antipsychotics in Very Simple and Very Detailed Steps
Very Simple Steps:
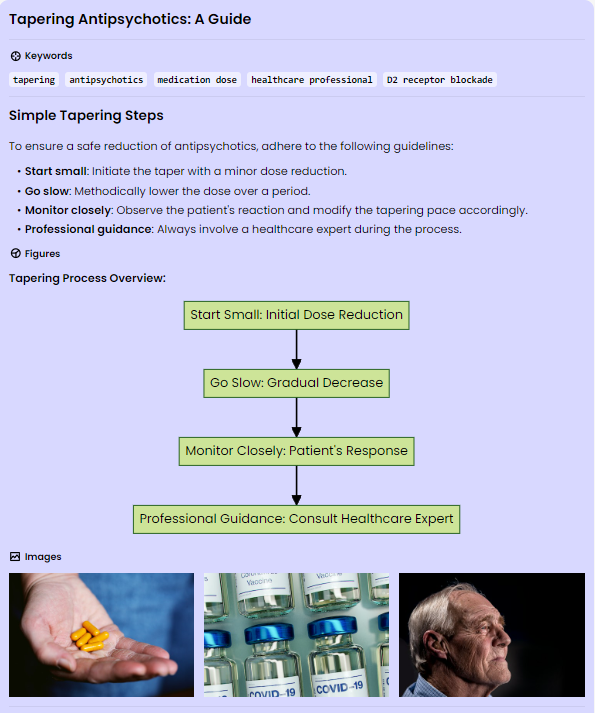
To safely taper antipsychotics, follow these simple steps:
1. Start with a small reduction in the medication dose.
2. Gradually decrease the dose over time.
3. Monitor the patient's response and adjust the tapering rate as needed.
4. Consult with a healthcare professional throughout the process.
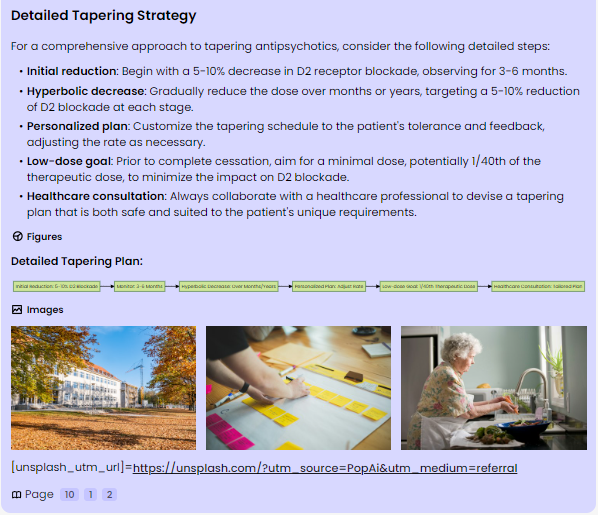
Very Detailed Steps:
1. Begin with an initial reduction of 5-10% of D2 receptor blockade and monitor the patient's response for 3-6 months.
2. Decrease the dose gradually over months or years in a hyperbolic manner, aiming for a reduction of 5-10% of D2 blockade at each interval.
3. Tailor the tapering plan to each patient's tolerance and response, adjusting the tapering rate based on individual needs.
4. Before complete cessation, aim for a very low dose, as small as 1/40th of the therapeutic dose, to prevent a significant decrease in D2 blockade.
5. Always consult with a healthcare professional to develop a safe and effective tapering plan tailored to the patient's specific needs.
What is the risk of relapse if the medication is withdrawn very gradually?
The risk of relapse when antipsychotic medication is withdrawn very gradually is significantly reduced. Evidence suggests that longer tapering periods, spanning months to years, are associated with lower relapse rates compared to more rapid tapering periods. Studies have demonstrated an inverse dose response between the duration of discontinuation and the rate of relapse, with longer tapering periods leading to substantially lower relapse rates. For instance, stopping antipsychotics over a period longer than 10 weeks resulted in a relapse rate of 31%, indicating a significant reduction in the risk of relapse with gradual withdrawal. Additionally, gradual tapering allows time for the reversal of underlying neuroadaptations, potentially minimizing the risk of relapse on discontinuation. This approach aligns with the principle of reducing the rate at which the equilibrium is disturbed, thereby mitigating withdrawal symptoms and reducing the likelihood and intensity of withdrawal psychosis. Therefore, a very gradual withdrawal of antipsychotic medication is associated with a lower risk of relapse, providing a strategic advantage in the management of discontinuation.
One reported that 48% of relapses occur in the first 12 months after antipsychotic discontinuation (40% in the first 6 months), with only 2% per year after this.' What it means 'only 2% per year after this?'
The statement "with only 2% per year after this" refers to the relapse rates following antipsychotic discontinuation. It indicates that after the initial period of 12 months, during which a significant proportion of relapses occur (48%), the subsequent annual relapse rate decreases substantially to 2%. This suggests that the risk of relapse diminishes significantly after the first year following antipsychotic discontinuation. In essence, the phrase "only 2% per year after this" signifies a notable reduction in the rate of relapse over time. It implies that the risk of experiencing a relapse diminishes considerably beyond the initial 12-month period, with a much lower annual relapse rate of 2% thereafter. This information underscores the importance of understanding the temporal pattern of relapse following antipsychotic discontinuation and highlights a significant decrease in the risk of relapse in the subsequent years.
Do relapse rates in the discontinuation group converge with those in the medicated group?
Yes, the document indicates that the relapse rates in the discontinuation group converge with those in the medicated group. The evidence from the document suggests that the discontinuation group generally shows more relapses than the maintenance (medicated) group in most studies examined. However, there are exceptions, such as studies with longer tapering periods or longer follow-up periods, which have shown no significant difference in relapse rates between withdrawn patients and those who were maintained on antipsychotics. For example, one study in people with first-episode psychosis with a tapering period of 10–40 weeks found no significant difference in relapse rates between withdrawn patients and those who were maintained on antipsychotics. Additionally, tapering over months and years demonstrated no significant difference in relapse rates between patients who continued or discontinued antipsychotics. Therefore, while the discontinuation group generally exhibits more relapses, there are instances where the relapse rates in the discontinuation group converge with those in the medicated group, particularly in studies with longer tapering periods or longer follow-up periods. If you have further questions or need additional details, feel free to ask.
The above results were obtained with the web tool PopAi: https://www.popai.pro/
Link to Original Research Paper: Method for Tapering Antipsychotic Treatment That May Minimize the Risk of Relapse | Schizophrenia Bulletin | Oxford Academic (oup.com)
Download the Original Research Paper in PDF: From Google Drive
😀🥰💞💘💓💕💗💙💚💛🧡💜💝